This is a simple technique that I have developed over the past many years that I have found to be extremely useful to help with the treatment of my patients. For me acupuncture is most exciting when you are able to evaluate techniques and points in real time and make immediate changes. And it’s often more interesting and engaging for patients as well. And this is a way to do that. It is simple to learn and can be used in combination with all of the other techniques you employ with your patients. Some of the features of it:
- It often forms the basis of the balancing work I do with patients.
- It helps refine diagnosis.
- It helps with point choice and fine tuning point location
- It helps with evaluating if the stimulation used was sufficient
- It provides another method for distal release of areas of tightness on people’s backs
I first was exposed to touching points to see how they affect other areas when I started to study with Kiiko Matsumoto. I was impressed with how one could find points that would make changes immediately and that you could “audition” points before you used them to assess their likely effectiveness.
Palpating the Shu points have become an important part of my diagnosis and treatment strategy. It has formed a reflex system similar to the Japanese acupuncture reflexes but it jives with the theory of TCM really well and helps to refine diagnoses and treatments. And the points identified with this method forms the foundation of points that I use to start a treatment to relax and balance a patient. And treating the points indicated by the Shu points will often lead to a better treatment outcome and easier time with the other points you want to include for other reasons, such as a local musculoskeletal problem.
In English we talk about these points as Associated points. Usually this is meant in the sense that these points are useful for the treatment of the organ that is associated with each of them. This is true, but another more important aspect of these points as I have discovered is their importance in diagnosis.
Usually the Mu points are spoken of as being the special points for palpatory diagnosis. And whereas they are useful, I find that they don’t react often unless things are really bad. Back Shu points, on the other hand are often very sensitive barometers of what is happening. Also they are dynamic and can change in their palpation quality very quickly and can, due to their dynamism, help you arrive at a diagnosis, choose points, and determine if your treatment is likely to be effective.
This dynamism is reflected by some of the sense of “Shu” in Chinese. When I asked Dr. Hong Jin about this, she told me that the word “Shu” of the back Shu has a meaning of transformation. These are the points where transformation happens. They are like switching stations in my view, nodes in the flow where the information on the associated meridian, energy system, or organ can become available for very easy evaluation. This dynamism of “transformation” is reflected in them having multi-functions in palpatory diagnosis and in the fact that they are extremely sensitive to quick change in how they feel.
And whereas I palpate the pulse, the hara, and the channels, I have found that palpating the Shu points has become the most powerful technique I have for diagnosis, point choice, likely efficacy of treatment, and teaching tool for bringing patients on board with the process. And the further beauty of it is that is nearly instantaneous, it’s feedback in real time.
Palpating a person’s Shu points has become an integral part of my intake. Sometimes I will go over all of them but often I will go to specific ones or general areas to check out something that I may have suspected from their history, symptoms, pulse, or other sign. I usually palpate the Shu points with the person lying on them. I know this sounds counterintuitive but since they are nearly the only points from the main channels on the back side of the body, it leaves the rest of the body available for confirmation and also for watching the reactions of the person on his or her face.
It takes a little practice doing it but it is easy enough to learn with a little practice. Can you do it with them prone? Sure, provided that you give them enough pillows to support them in the right places so that their back is really relaxed. That’s another advantage to happen the person lying supine. With them on their back and the knees lightly supported, the back should be doing absolutely nothing, so that any areas of tightness stand out and are, from my perspective, significant.
How to get under them? First form your hands like a blade, fingers together and stiff. At the upper part of the back and often at the lumbar area one can often get your fingers to the Shu points directly by essentially shoving them under the person, perhaps with compressing down the foam on the table with your knuckles as you are going in. You’ll want to keep your four fingers together for this.
The middle and lower thoracic Shu points can be more challenging. A good technique for getting into position there is to take your blade hands and place them palm down on the table with the thumbs tucked under their body as much as you easily can. Then lift their body up slightly with the posterior thumb while at the same time supinate and ulnar deviate at the wrist, thus flipping your hand over. And if you do it right, your fingers will land just about right on top of the inner Bladder line. And you can also use your non-palpating hand to gently lift up the edge of the person’s body, allowing the other hand to slide underneath.
Once your hand is underneath, feel for the bundle of paravertebral muscles. Or go to the spine and then pull back toward you about two inches. What you are looking for are areas of tightness that stand out from the areas above and below the area of tightness. You can curl your fingers of your palpating hand to strum across the muscles. Or another method that works better for some people is to put the four fingers together with the fingers in a fixed position with the fingers slightly curved, and, rather than actively curling the fingers, rock the fingers across the muscle bundle using the knuckles of the hand at the metacarpal-phalangeal joints as a fulcrum.
So how do you know where you are?
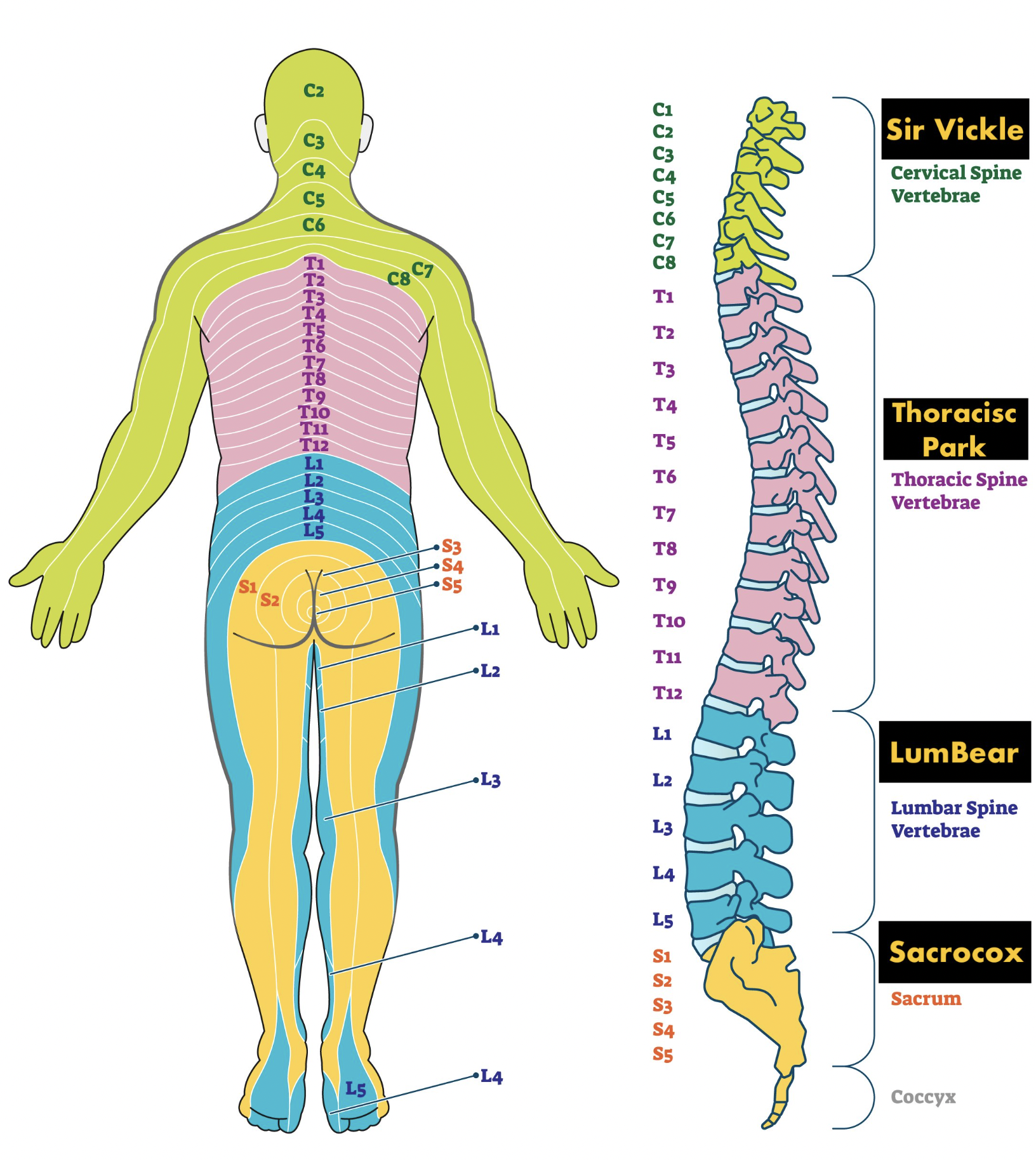
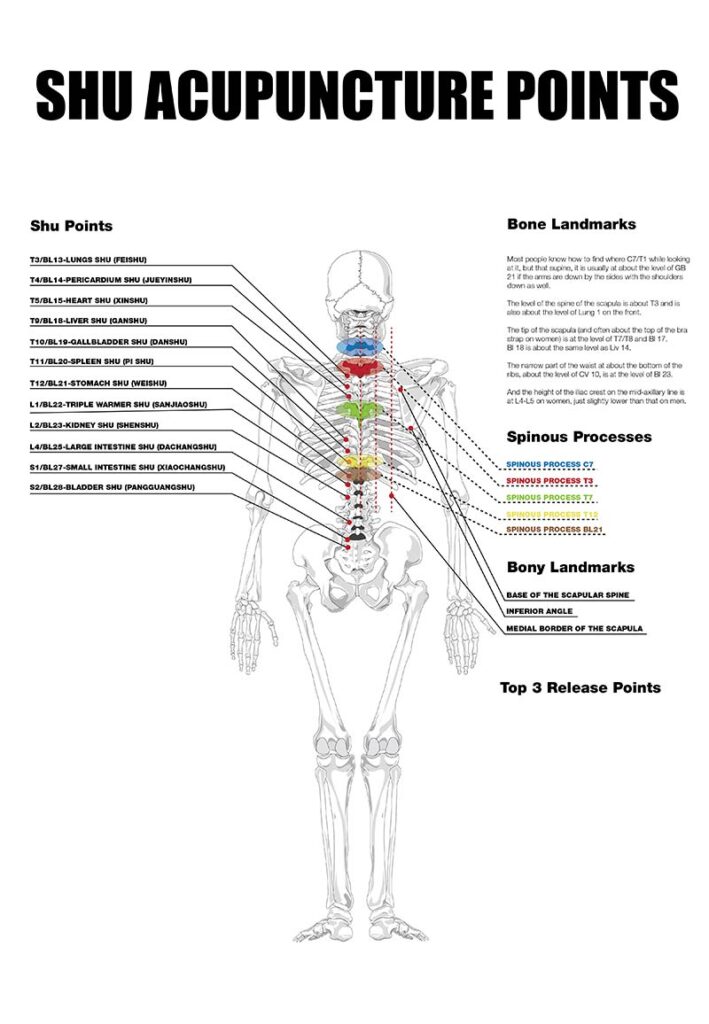
Most people know how to find where C7/T1 while looking at it, but that supine, it is usually at about the level of GB 21 if the arms are down by the sides with the shoulders down as well.
The level of the spine of the scapula is about T3 and is also about the level of Lung 1 on the front.
The tip of the scapula (and often about the top of the bra strap on women) is at the level of T7/T8 and Bl 17.
Bl 18 is about the same level as Liv 14.
The narrow part of the waist at about the bottom of the ribs, about the level of CV 10, is at the level of Bl 23.
And the height of the iliac crest on the mid-axillary line is at L4-L5 on women, just slightly lower than that on men.
Between these landmarks you can easily interpolate. Or if you prefer you can actually count the vertebra. It sounds hard but it is a pretty doable with a little practice.
So when you palpate what should you do exactly and what are you looking for? Generally you are looking for areas of notable tightness, the really tight areas will be very dramatic, both to your palpation and to the patient. Many times the patient will have no ideas that the area in question is so tight or sensitive. When the tension is moderate or more subtle, one can bend at the metacarpal-phalangeal joints with the still straight fingers, and in doing so, lever your fingers up into their muscles over the Shu points using the knuckles as a fulcrum. Then you can take the fingertips and strum the muscles from medial to lateral and back for further clarification.
Think of having a conversation with each Shu point you’re testing. “Ask” the point, “How is this?” by your palpation and listen to its response as you look for points to release it.
Most of the time, you will have no doubt as to what is significant. You will clearly feel it and so will the patient. And that’s part of the beauty of it. Both you and the patient will be clear that something funky is going on there. And if you do your work properly, palpating, watching and listening to them as you proceed with this, both of you will know after your treatment that something changed in a positive direction.
Have them practice trying to locate.
Now once you’ve found the tight areas, what do you do with them? While keeping contact with the tight Shu point with one hand, palpate points with the other hand to evaluate the effectiveness of that point for balancing and releasing that localized area of tightness. For most of the areas that we will find, the points that will best release them will be on the associated meridian of the Shu point.
Palpating the points to determine their effectiveness for Shu point release does not need to be done very firmly. And as you get better with this, you just need to just touch the individual point to properly assess its utility. The release sensation on the Shu point with usually happen within a second or two of contacting the appropriate point on the meridian with the other hand. There are a few people I have seen that it takes their body a few seconds more to react, but this is not common. The release you may feel in the Shu points may often not be complete, but when you find the right one you will feel a significant softening of the Shu point. This is what you are looking for with this method.
You ever learn alternate locations of points on the body? With this technique you can audition the various locations to see which is most effective for the person at the particular time you are seeing them. You can also evaluate what angle to insert the needle to have the best effect by giving a vector to your palpation of the release point.
The most effective point will change, depending on the day. It seems like this method will often key into the point that is “open” on a particular day. And somedays it will seem like many people will have the same point that is effective on a particular morning for a particular Shu point. There are systems that attempt to find the point that is open on a particular day and time of day. Some days it will seem like you are keying into this.
And by the points that are most effective, you can hone a diagnosis. Let’s take an example. You have a patient with a Liver pulse that is somewhat wiry but is also empty when you press into it. The sides of the tongue are pale, but the tongue sides are pulled in giving the tongue a spatulate appearance. They have other signs that point to both Liver Blood deficiency as well as Liver qi constraint. Well, each of those diagnoses can lead to the other condition. How can we determine which is the most important feature to focus on during today’s treatment?
You go to Bl 18 and find a notable tightness there and then with your other hand, you start palpating points on the Liver channel. If points like Liver 8 and Spleen 6 are the points that release Bl 18, it indicates that treating the deficiency is the most important thing to address today. If a point like Liver 4, 5, or 14 releases Bl 18, moving the qi is the most important focus for today’s treatment. And this can help you skew the focus of your herbal formula that you might give them at that treatment.
Shu Points and the distal points most often useful for the Shu point release
The points for release of the Shu points I focus on are most often are the points distal to the elbow and the knee. As you know from your studies, these are very powerful points, in general. They often have special functions as elemental points according to the five phases. They also have functions according to the delineation of jing well, Shu stream, he sea points, etc. These points prove to be the effective point for Shu point release about 70% of the time. About 15% of the time, the effective point will be a point in the upper arm or thigh. And another 15%of the time, the effective point will be on the trunk of the body.
Let’s go over the various Shu points and the most likely points to look at for release. I will try and list the points with the ones most often effective listed first.
Bladder 11 is a point that I don’t find much utility so far.
Bladder 12 is the wind Shu point. This will get tight when someone has an acute wind invasion. But it will also be tight with someone who got sick some time ago and never fully recovered. This person may have “retained pathogen”. This will provide a diagnostic clue as to this phenomenon and also guide you to points that may best release this.
So which points do you suspect would be most effective? L7, LI4, TH5, GB 31, GB20. Test them out to see which one is best.
Bladder 13 is the Shu point for the Lung. The most effective points are often L7, L5, L9, and sometimes L1, 6. Occasionally L3 (often with someone with retained grief) or L 8
Bladder 14 is the Shu point for the Pericardium. The most effective points tend to be P6, P3. Sometimes look to P5, P7, and occasionally P1
Bladder 15 is the Shu point for the Heart. The most effective points tend to be H3, 7. Also look to H9, especially with someone with Heart Blood deficiency (it’s the tonification point). And occasionally it can be H 6 or 5.
A special note about the upper jiao and about the Shu points in general. Sometimes when you feel a tightness at a Shu point and you can’t find a good point to release it, the tightness you feel may, in fact, be bleeding over from an adjacent Shu point that you didn’t yet notice or perhaps you may have mismeasured your location. And one of the things that I have noticed is in the upper jiao area, in particular, is that there seems to be more bleed over among the Lung, Pericardium, and Heart. That is, you may be pretty sure you are on a Lung Shu point and the effective release point is a Pericardium point. Perhaps this is because they are all affected by the zong qi generally.
Another note is that the outer Shu points are also diagnostic and can be found to be released by the points associated with the inner Shu points. Thus Bl 43 can be released by a point such as P6. And this upper jiao bleed over can be seen in the outer Shu points as well.
Bladder 17 is the Diaphragm Shu. Tightness here will often be accompanied by infracostal tightness in the belly. The best point for releasing this tightness and the diaphragm is the Ear Diaphragm point. Also useful is Stomach 20.
Bladder 18 is the Liver Shu point. The most common points for release are Liver 3, Spleen 6 (because it is also on the Liver channel), and Liver 8. Also effective are Liver 4, 5, 13, and 14, and occasionally Liver 2.
Bladder 19 is the Gall Bladder Shu point. The most common points for release are GB 41, 34, 36, and Dang Nan Xue. Also effective are GB 40, 31-32. Sometimes look to GB 42, 39, 38, or 37 for release of Bl 19.
Bladder 20 is the Spleen Shu point. The most common points for release are Sp 6, 4, 10. Also effective are Sp 9, 8, 3. Rarely Sp 2 or even Liver 13 (it’s the front Mu of the Spleen).
Bladder 21 is the Stomach Shu point. The most common points for release are Stomach 36, Lan Wei, 40, and 37. Also useful to try are St 42, 43, 34.
For the Liver and GB, sometimes I’ll find that it’s an area encompassing both Shu points, so one needs to check both meridians for the release point. Similarly one will find this on the Spleen and Stomach. You’ll focus on one them as being the primary area of interest when actually the release is to be found on the paired meridian.
Bladder 22 is the Triple Heater Shu point. The most common points for release are TH 9, TH5, and TH3. Also effective are TH 6 and TH4 and occasionally TH 8.
Bladder 23 is the Kidney Shu point. The most common points for release are K7, K2, K 10. Also useful is K3 and K 6 and sometimes Sp 6.
Bladder 25 is the Large Intestine Shu point. I have not found many times that the LI points are effective. In fact, once we get to the lumbosacral region a special relationship seems to hold forth.
This region, along with the upper shoulder and neck region, is so often an area of discomfort in our patients, from a purely musculoskeletal perspective. And each of these two areas seems to have some special associations that are helpful to keep in mind.
The meridian that seems to rule the sacrum, in my experience, is the Gall Bladder channel. The internal pathway of the Gall Bladder channel courses through the sacrum and the most effective points to relieve the tightness and discomfort there are the points mentioned in the Gall Bladder section above.
I’ll give you some ideas for release of the other special area of the upper shoulders and neck. One of my teachers used to say that L7 is the master point for treating the neck area. This point can be remarkably effective, but many times you may need to use and alternate location or a specific angling. We will talk about this in the next section. Many times the area that is tight and needs release is the SI 15 up into the bai lao area (on the Bladder channel). The most effective points tend to be SI 3, 7, 6. Or the area of discomfort is around TH15, in which case the point to look at could be TH 3, 5, 9, etc. Another point to look at for this area is the motor point for the flexor carpi ulnaris. This point is special for the tightness that so often happens at the attachment of the levator scapula. It is located at one third of the way from H3 to H 7.
And L7 angled toward L8 can be a special point for the anterior scalenes.
Variant Point Locations
One of the uses of this Shu point system is the ability is gives you to find the most effective location of a point for a particular person on a particular day. If can even help you find the best angle to insert the point.
I’d like to share with you some of the locations for some of the above mentioned points that I have found useful in my years of practice. Some of them may seem strange compared to what is currently taught. But in fact, some of them were taught in these alternate locations when I studied many years ago. Others are ones that I have discovered in my poking around the past many years.
Let’s follow our outline from above regarding the Shu points and go from the top down and I’d like to point out some locations I like.
Lung
So for the Lung points, Lung 7 I most often find in line with L 9, just proximal to the radial stylus. I’ll often needle it from radius to the ulna.
But sometimes, especially for the neck region, I’ll find it most effective when it’s needled from this location toward L 8.
So how do you audition various angles? Place your finger on the point and traction it in a particular direction that you may want to needle it. You will sometimes find that a particular direction will give a much better effect.
I will sometimes locate L5 more lateral, in what some people call Japanese L5. And sometimes angling this point toward L6 will give the best release.
And speaking of L 6, I tend to find it just distal to the flexor muscle bundle in the hole on the anterior surface of the radius. This is the xi cleft point and can be a dandy point. And for L 1 I will often palpate around an area a little bigger than a quarter to find the most effective location.
Heart
For the Heart points I think I start with the points on the forearm at a different location than many of you. I start with H 7 on the wrist crease on the radial side of the pisiform. You can feel the hole there and then there are three more holes going up the forearm each a half cun apart. And when you get to H4, that’s the last hole you will feel.
Triple Heater
On the Triple Heater, I will check TH4 on either side of the extensor tendon to see if one is more effective than the other. And for TH 9, the location I am most likely to find effective is a Japanese location about two-thirds of the way from TH4 to LI 11 in a hole there.
Liver
For the Liver points, I will look for Liver 4 on both sides of the tendon. The preferred location is medial to the big tendon, but many times I will find the effective location is just lateral to the tendon and can be sometimes best used with an angle proximally.
Liver 5 I will check on the bone where you are taught, but more often I find it effective in the hole just medial to the bone.
Liver 8 I will often audition several locations, but my most dependable location is in the big hole proximal to the medial knee.
Liver 13 I like to find at the anterior inferior corner of the eleventh rib.
Liver 14 I like to find in the 6th costal interspace, but more lateral than many of you find it. The location I like tends to line up with the lateral edge of the areola on men. It is also at the angle where the rib changes direction. There is a hole there and is often tender. The angle I favor there is angling it laterally between the ribs (sort of toward the axilla).
Gallbladder
For the Gall Bladder, I most often find GB 39 on the anterior surface of the fibula. You slide your thumb up the fibula to where it stops as the fibula dives under muscle. One of my earliest teachers said that one the names of this point is “no bone”. And I’ve found that a number of people that were trained many years ago were taught to find it here.
GB 34 can be in a variety of locations, but one of my favorite locations is to take the prominences of the tibia and fibula and make an equilateral triangle with GB 34 being the third point. When I am looking at Gb 31 or 32 as a location to release Bl 19 or the sacral area, I will sometimes palpate with three fingers, and then if I get a release, find out which of the three locations is best.
Spleen
On the Spleen, one non-standard place to check is just a little proximal to Sp 3, in the hole just proximal to Sp 3, in what some of the Japanese acupuncture people such as those studying with Kiiko Matsumoto call Sp3.2.
Kidney
For the Kidney, I will often locate K2 in a hole just inferior and posterior to the navicular. For K 6 I will look between the two tendons just inferior to the malleolus (and often needle it posteriorly), but I will also check a location about one cun inferior to that.
On K 7 I will often check an angle I learned from Dr. Tran. Sometimes the magic angle is one that he says he uses regularly, which is to angle the insertion anteriorly toward K8. And for K 10 the location that I find most often works the best is one that is one to two cun proximal to the popliteal crease, in the hole between the two hamstring tendons. This location seems to be particularly effective.
Checking your work
One of the nice features of this system is to go back and quickly check your work. That is to say, go back and repalpate the Shu points you found to be noteworthy. Sometimes you will find that one of the points has not released well. What this usually means is that you need to back and give the release point some additional stimulation. Or sometimes you need to try a different angle. And for extra effectiveness, leave your one hand on the Shu point and lightly tickle it while stimulating the distal point.
Some patients, who were aware of the tight spots when you started, will be amazed at the changes that have happened immediately.
What to do when all of the Shu points seem tight
Occasionally you will have a patient whose whole paravertebrals are like cables. It’s hard to differentiate any stand-out tight area. What I will often do with these patients is to use the Master and Coupled points for the Du Mai, SI3 and Bl 62. And if you have a set of Japanese ion pumping cords, put the black clip on SI3 and the red on Bl 62 and maybe add the ear Shen Men point. Let these points rest for maybe 10 minutes or so. Almost always when you come back, the generalized tightness will have dissipated and the field will have cleared so that you can find the key areas for treatment.
Flow of treatment session when using the Shu point system
It doesn’t replace what you have normally done. It provides you with another tool to evaluate and come up with effective treatment for your patient. For me, I may not examine the pulse in detail or check the tongue at each and every treatment. But I usually will examine the abdomen and check the Shu points at each treatment. I will palpate the hara to see if there is an extra meridian or other finding that is standing out that may be important in the first set of needles is use. And several points from my Shu point findings will often be a part of my first set of needles. And with the Shu points I will often scan for one noteworthy finding in the upper, middle, and lower jiaos. I won’t always find one, but I do scan in that way.
And then in my second set of needles there may be points that I know to be effective for a condition from my TCM training or other information. Or if it’s a musculoskeletal problem, I will probably have done some manual muscle testing to inform what points might be most effective for treating that condition and I will include them then. But of course, if they have some sort of back pain, the work that was done with the Shu point system, will have already gone a long way toward diffusing the congestion in the area of their back that they are having trouble in.
Of course there is a good deal of variability in how I work, but this gives you an idea of how the flow might likely go when I’m seeing a patient.
I hope this material will prove useful to you in your practice. Try it out. Experiment with it. You will probably make further refinements with it that will suit you and the way you practice. I think you will find it useful and interesting to incorporate. Let me know if you find it useful.